
Cologuard v2 results and what it means for the future of cancer screening
Are the results good enough for an inflection point in colorectal cancer screening?

We will cover what the results of the EXAS 0.00%↑ Exact Sciences Cologuard v2 trial BLUE-C mean, and how they compare to GH 0.00%↑ Guardant Health SHIELD and ILMN 0.00%↑ GrailBio/Illumina Galleri.
But first, we give a perspective of where we are in Liquid Biopsy for Cancer Screening or Early Detection (LQED).
What’s the deal with Liquid Biopsy Cancer Screening?
Liquid biopsy is a type of cancer screening test that uses a blood sample to detect cancer cells or DNA fragments from cancer cells. It is a less invasive alternative to traditional cancer screening tests, such as colonoscopies and mammograms.
There are several reasons why liquid biopsy is being considered for cancer screening:
It is less invasive than traditional cancer screening tests. Liquid biopsy does not require any surgery or imaging, which can make it more appealing to patients.
It can be used to screen for multiple types of cancer. Some liquid biopsy tests, such as the Galleri test, can be used to screen for up to 50 different types of cancer. This makes them a more efficient way to screen for cancer than traditional cancer screening tests, which are only designed to detect one type of cancer.
It can be used to monitor cancer patients. Liquid biopsy can be used to track the progress of cancer in patients who have already been diagnosed. This can help doctors to determine whether the cancer is responding to treatment or if it is spreading.
There are a number of liquid biopsy tests that are currently available or in development. Some of the most well-known liquid biopsy tests include:
Galleri test (Grail Bio): This test can detect up to 50 different types of cancer from a single blood draw.
Guardant Health SHIELD screening assay: This test can detect colorectal cancer from a single blood draw.
Exact Sciences Cologuard (Version 1) assay: This test can detect colorectal cancer from a stool sample. It is informally known as the “poo-in-a-bucket test”.
A new generation of liquid biopsy assays is also in development. These assays are designed to be more sensitive and specific than current liquid biopsy tests. They are also designed to be able to detect cancer earlier, which can lead to better outcomes for patients.
Some of the companies that are developing new liquid biopsy assays include:
Freenome: This company is developing a liquid biopsy assay that can detect early-stage colorectal cancer based on a multi-omics approach.
Natera: the company is also allegedly working on LQED methods.
Burning Rock Biotech: the company is working on LQED methods in clinical trials mostly located in China and South East Asia.
Singlera Genomics: the company already has results for small sample size trials.
EarlyDx: the company already has results for small sample size trials.
Avida Biomed (now Agilent): the company already has results for small sample size trials.
Delfi Diagnostics
Bluestar Genomics
Many others…


Liquid biopsy is a promising new technology for cancer screening. It is less invasive than traditional cancer screening tests and can be used to screen for multiple types of cancer. However, more research is needed to determine the accuracy and effectiveness of liquid biopsy for cancer screening.
What is the desired specificity of a cancer screening assay?
Specificity is a measure of how well a test correctly identifies people who do not have the disease. In other words, it is the proportion of people who test negative who actually do not have the disease.
For a cancer screening assay, a good specificity would be in the range of 95% to 99%. This means that for every 100 people who test negative for cancer, only 1 to 5 of them will actually have the disease.
A cancer diagnostics assay, on the other hand, does not need to have as high a specificity as a cancer screening assay. This is because a diagnostics assay is only used after a person has already been identified as being at risk for cancer. Therefore, the false positive rate of a diagnostics assay is less important than the false negative rate.
A good specificity for a cancer diagnostics assay would be in the range of 80% to 90%. Specificity answers of 100 people who don’t have cancer, how many have a negative test.
Specificity and Negative Predictive Value
I should clarify upon request of a reader the difference between Specificity and Negative Predictive Value (NPV). NPV is a statistical measure used in medical diagnostics and research to assess the accuracy of a diagnostic test in correctly identifying individuals without a particular condition. NPV is the probability that a person does not have the condition given a negative test result.
On the other hand, specificity is a measure that indicates the proportion of true negatives among all the individuals without the condition. It is the ability of a diagnostic test to correctly identify individuals who do not have the condition.
The key difference between NPV and specificity lies in how they are influenced by the prevalence of the condition in the population being tested:
1. NPV and Prevalence: NPV takes into account both the sensitivity and specificity of the test as well as the prevalence of the condition in the population. The prevalence of a condition is the proportion of individuals in the population who actually have the condition. NPV is affected by prevalence because it considers the likelihood of encountering true negatives in the population. As the prevalence of a condition increases, the probability of encountering a true negative decreases, which in turn reduces the NPV. In other words, as the prevalence increases, the NPV tends to decrease.
2. Specificity and Prevalence: Specificity, on the other hand, is not directly influenced by the prevalence of a condition. It is solely determined by the test's ability to correctly identify individuals without the condition, regardless of how common or rare the condition is in the population. The formula for specificity does not include prevalence in its calculation, so it remains constant regardless of changes in prevalence.
—
Back to the numbers. Here is a table that summarizes the difference between specificity for cancer screening assays and cancer diagnostics assays:

The reason why cancer screening assays need to have a higher specificity than cancer diagnostics assays is because cancer screening assays are used to screen large populations of people. If a cancer screening assay has a low specificity, then a large number of people who do not have cancer will be falsely identified as having cancer. This can lead to unnecessary anxiety and medical interventions.
Cancer diagnostics assays, on the other hand, are only used after a person has already been identified as being at risk for cancer. Therefore, the false positive rate of a diagnostics assay is less important than the false negative rate. This is because a false negative result means that a person who actually has cancer will be missed. This can lead to delays in diagnosis and treatment, which can have serious consequences.
What about GrailBio Galleri?
The reason why cancer screening assays need to have a higher specificity than cancer diagnostics assays is because cancer screening assays are used to screen large populations of people. If a cancer screening assay has a low specificity, then a large number of people who do not have cancer will be falsely identified as having cancer. This can lead to unnecessary anxiety and medical interventions.
Cancer diagnostics assays, on the other hand, are only used after a person has already been identified as being at risk for cancer. Therefore, the false positive rate of a diagnostics assay is less important than the false negative rate. This is because a false negative result means that a person who actually has cancer will be missed. This can lead to delays in diagnosis and treatment, which can have serious consequences.
Here is a table that summarizes the difference between specificity for the Galleri test and Cologuard v1:
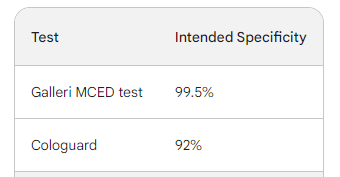
As you can see, the Galleri test has a significantly higher specificity than Cologuard. This is because the Galleri test is designed to detect a wider range of cancer types and is used to screen large populations of people.
When are these tests going to be widely used?

MCED tests are able to detect multiple types of cancer from a single blood draw. This is in contrast to single-cancer tests, which can only detect one type of cancer. MCED tests have the potential to reduce cancer mortality by 15% if they are adopted by a large number of people.
The cost of goods sold (COGS) for an MCED test has fallen by more than 90% over the past five years. This means that the cost of producing an MCED test is now very low. As a result, MCED companies can generate positive gross profit even if they are reimbursed at a price of $500 per test.
Currently (June 2023), the price out of pocket of the GrailBio Galleri test is double that amount, at $949.
Will vendors strive to have more sensitive tests or more profitable tests?
Test designs are becoming more efficient, which means that MCED companies can add more sensitivity and/or profitability for each incremental dollar in cost. This gives MCED companies the incentive to focus on improving the sensitivity of their tests, as this will lead to more lives saved.
Why would vendors opt for the former?
There are two main reasons why vendors would opt to improve the sensitivity of their MCED tests:
To save lives: The more sensitive a test is, the more likely it is to detect cancer early. Early detection is critical for cancer survival, as it allows for treatment to begin before the cancer has spread.
To increase profits: A more sensitive test will lead to more patients being diagnosed with cancer. This will increase the number of tests that are sold, which will lead to increased profits for the vendor.
In addition to these two reasons, vendors may also opt to improve the sensitivity of their MCED tests in order to gain a competitive advantage. If a vendor's test is more sensitive than the tests of its competitors, then it will be able to attract more patients and generate more profits.
Overall, there are a number of reasons why vendors would opt to improve the sensitivity of their MCED tests. These reasons include saving lives, increasing profits, and gaining a competitive advantage.
Cologuard v2 BLUE-C results
Exact Sciences announced on Tuesday that the new version of its Cologuard colorectal cancer detection test met all endpoints of its BLUE-C study and showed improvement over the first generation of the test across all topline metrics, including a 30 percent lower false positive rate.
The BLUE-C study was a multi-center, prospective study of more than 20,000 adults aged 40 years and older who were tested with the improved, multi-target Cologuard assay. The results of the study were compared to patients' colonoscopy findings.
The company reported that test specificity improved to 91 percent in the study, while sensitivity rose to 94 percent for cancer and 75 percent for high-grade dysplasia.
Since specificity is a measure of how well a test correctly identifies people who do not have the disease, it is the proportion of people who test negative who actually do not have the disease.
Behind the curtain, we analyse what this means for the other players in the field…